PDA Closure in Dogs and Cats
Minimally invasive treatment of patent ductus arteriosus
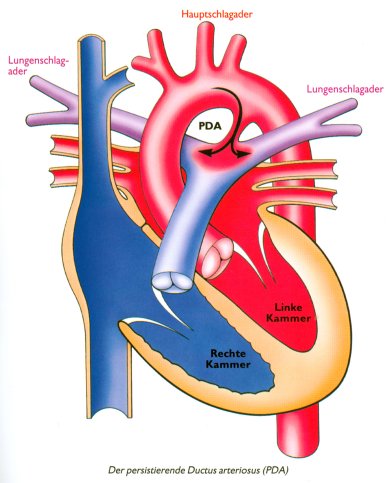
This page focuses specifically on the treatment of patent ductus arteriosus (PDA) in dogs and cats.
If you are looking for more general information about the disease itself, symptoms, diagnosis and echocardiography, please visit our PDA disease page.
In most patients, a PDA should be closed as early as possible before irreversible cardiac or pulmonary vascular changes develop.
Why should a PDA be closed?
Closure eliminates the abnormal blood flow between the aorta and pulmonary artery and helps prevent progressive cardiac overload.
Main goals: reduce volume overload, prevent heart enlargement and improve long-term outcome
Important: intervention is usually recommended before severe secondary changes occur
How is PDA treated?
In the past, treatment often required open thoracic surgery. Today, many PDA can be treated by a minimally invasive catheter-based procedure.
This approach is much less invasive because the chest remains closed. In suitable patients it is therefore often the preferred option.
The exact closure technique depends mainly on patient size, vessel diameter and the anatomy of the ductus.
Standard method: Amplatzer Duct Occluder
The Amplatzer Duct Occluder is now one of the most commonly used devices for interventional PDA closure.
This self-expanding nitinol device is delivered through a catheter and positioned within the ductus. In many suitable patients it allows very reliable closure with a low complication rate.
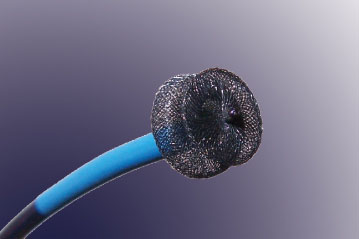
Its specific shape and retention skirt help stabilise the device in the ductus. The internal fabric also supports permanent occlusion.
How is the procedure performed?
For catheter-based PDA closure, a catheter is advanced through the femoral artery to the heart. Before the closure device is deployed, angiography is commonly performed to define the exact shape and size of the PDA.
The appropriate closure device is then positioned under imaging guidance.
 Catheter-based PDA intervention performed at LMU Munich
Catheter-based PDA intervention performed at LMU Munich
Angiography before closure
Contrast angiography helps visualise the ductus precisely and supports the selection of the most appropriate closure system.
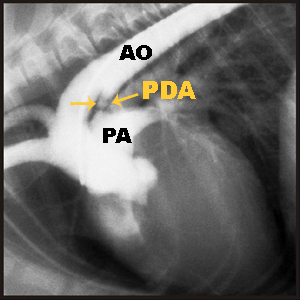 The PDA is visualised by contrast injection.
The PDA is visualised by contrast injection.
AO: Aorta
PA: Pulmonary artery
Video of angiography before PDA closure:
Angiography of a patent ductus arteriosus before closure, demonstrating abnormal contrast flow from the aorta into the pulmonary artery.
Which patients are suitable for Amplatzer closure?
In many cases, the Amplatzer technique can be used successfully in patients weighing approximately 2.0 to 2.5 kg or more.
However, suitability depends not only on body weight, but also on vascular access size and ductal anatomy.
Alternative option in smaller patients: coil closure
In smaller patients or in selected anatomical situations, coil embolisation may be used instead of an Amplatzer device.
The coil is delivered through a catheter in a stretched configuration and takes on its spiral shape once released. It can be positioned carefully before final detachment.
 Coil design and associated thrombosis contribute to permanent occlusion of the ductus.
Coil design and associated thrombosis contribute to permanent occlusion of the ductus.
After deployment, echocardiography and sometimes repeat angiography are used to assess how complete the closure has become.
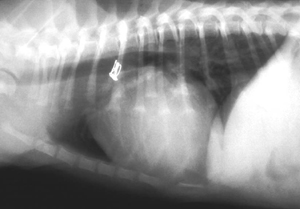
Angiography after successful coil closure:
Post-procedure angiography showing no relevant residual flow through the ductus after closure.
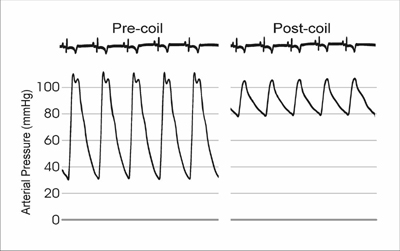
What happens to blood pressure after closure?
In patients with an open PDA, the diastolic arterial blood pressure is often markedly reduced. After successful closure, an immediate increase in diastolic pressure can often be observed.
When is surgical closure needed?
Surgical PDA ligation may still be recommended in very small patients or when vascular access or ductal anatomy is not suitable for a catheter-based procedure.
In surgical closure, the chest is opened and the ductus is ligated directly or closed with a vascular clip. Because catheter-based treatment is usually less invasive and highly effective, surgery is now generally reserved for selected cases.
Why is echocardiography important before intervention?
Echocardiography is essential for planning the procedure. It helps assess the anatomy of the ductus, the volume overload of the heart, and whether pulmonary hypertension or a right-to-left shunt may already be present.
Patients with pulmonary oedema should be medically stabilised before intervention whenever necessary.
Prognosis after successful PDA closure
If closure is performed successfully and before irreversible secondary changes occur, prognosis is usually excellent.
Many patients can go on to have a normal life expectancy. In some cases, medication can later be reduced or discontinued.
Estimated cost
The total cost of PDA closure, including diagnostic work-up, varies by clinic. A rough range is often around EUR 2,000 to 3,500 or more.
Further information and referrals
For general information about the disease itself, symptoms and diagnosis, please also read our PDA disease page.
For case discussion, appointments or referral enquiries: kleintier.kardiologie@lmu.de